Late last year, a study was published that really brought surprising findings about how your brain can store and program an immune response.
For decades, it was thought that the Brain and the immune system operated independently from each other, but research in the past 20 years have put that idea to rest.
How the brain can regulate immune function has been largely unknown. Does it happen as a by product of neuro-endocrine regulation, or can higher neural centers in the cerebral cortex play a role?
Koren et al did a really interesting study published last year that showed an area of the brain called the insular cortex may actually store and trigger very specific immune responses.
Their team took mice and gave them either a lab induced form of colitis or peritonitis. Both conditions will cause abdominal pain and inflammation, but in very different ways. Colitis will cause inflammation within the digestive organs while peritonitis will cause inflammation outside of the organs.
The researchers showed that colitis and peritonitis produced unique signatures of activation on the area of the insular cortex in mice.
Using some advanced techniques, they were able to specifically turn on the same neurons that were activated during the colitis or peritonitis flares.
They found that turning on those pattern of neurons in the brain reproduced a similar immune response in the guts of the colitis or peritonitis model 🤯
This is remarkable because it suggests that the brain may keep a map of different immune patterns like it keeps a map of your body parts and the space around us.
The implications are interesting because what it opens the possibility that some inflammatory pain issues have a brain-based cause.
Something may start as an immune disorder like rheumatoid arthritis or spondyloarthritis, but plasticity may encode these responses in a way that it gets turned on without a trigger.
Could this be a bridge for how autoimmune disorders and plasticity become entangled creating chronic pain issues?
https://chiropractickeystone.com/wp-content/uploads/2022/03/1-1.png10801080Dr. Jonathan Chunghttp://chiropractorwellington.com/wp-content/uploads/2019/02/neuroplasticity-web.jpgDr. Jonathan Chung2022-03-15 17:19:242022-03-15 17:19:24Can Your Brain Program an Immune Response?
The brainstem is arguably the most important area of the brain in terms of keeping us all alive. Most medically educated people know that the Brainstem is tied heavily towards our ability to breathe and maintain heart rate.
But the Brainstem does so much more! It’s a bottleneck point for neural transmission the entire body, so lesions of the Brainstem can impact any other part of the body.
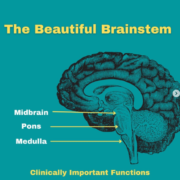
When we look at the function of the Brainstem, we usually separate the anatomy into 3 regions.
• Midbrain
• Pons
• Medulla
By knowing the function of each region, we can examine a patient and get a sense for any possible dysfunction, especially when we evaluate a patient’s cranial nerves.
A patient with impaired ability to move their eyes up and down may have midbrain dysfunction. A patient with issues with their face/jaw may have a problem at the Pons. A patient with nausea signs and balance problems likely has issues in the medulla.
By understanding these issues, it can help us see if a patient has a serious , life threatening issue that needs special tests or referrals. It can also help us design rehab for patients if these issues aren’t pathological.
Either way, looking at the anatomy and physiology of the Brainstem can create a sense of awe, as you understand that this small chunk of brain is responsible for so much of what makes us alive.
https://chiropractickeystone.com/wp-content/uploads/2021/10/the-beautiful-brainstem.png578597Dr. Jonathan Chunghttp://chiropractorwellington.com/wp-content/uploads/2019/02/neuroplasticity-web.jpgDr. Jonathan Chung2021-10-14 15:41:182021-10-14 15:43:22The Beautiful Brainstem
Our brains are made up of gray matter and white matter.
Gray matter is made up of pools of neurons that are responsible for specific tasks.
White matter is made up of axons which carry the information from our neurons to another region of the brain or body.
When we look at how chronic pain changes our brains, multiple MRI studies have shown that size of gray matter in our brains decrease. This is observed in parts of the brain that are associated with the painful body region, but it also affects other areas of the brain that affect us emotionally and cognitively.
We don’t necessarily know the exact implications of this, but it’s been suggested that decreased gray matter may be associated with decreased functionality of those brain regions. This is mostly driven by aging research where decreased gray matter is associated with declining cognition.
This may be a mechanism for how chronic pain can have downstream affects on cognition, autonomic function, and depression.
The good news is that these changes in gray matter are actually reversible!
Studies have shown that when pain is reduced or eliminated, some of these brain changes actually start to increase again.
We know that pain has a functional purpose in the acute phase, but chronic pain can be quite detrimental.
While we can’t always rid someone of pain, having the ability to reduce pain and the consequences of pain is really important. It’s also really important to develop emotional and cognitive strategies to best manage painful syndromes as well.
https://chiropractickeystone.com/wp-content/uploads/2021/10/chronic-pain-changes-brain.png598598Dr. Jonathan Chunghttp://chiropractorwellington.com/wp-content/uploads/2019/02/neuroplasticity-web.jpgDr. Jonathan Chung2021-10-14 13:56:292021-10-14 13:56:29Chronic Pain Structurally Changes our Brain
There’s some confusion about the functions of the two sides of the brain, so let’s talk about some myths and facts about brain hemisphericity.
We know that the the brain is organized into right and left hemispheres, but do these hemispheres have unique functions?
One of the most common beliefs is that personality traits are left or right brained. It’s typically thought that the left brain is for logic and problem solving, while the right brain is for creativity and spontaneity. Therefore people can train their left Brain by doing math, and train their right brain by doing art.
Verdict: 𝗙𝗮𝗹𝘀𝗲
A number of studies have found that logic and creativity tasks tend to light up both sides of the brain. Additionally, the brains of very creative or very logical people don’t tend to show much difference from one side to the other.
Now in #functionalneurology we do look for differences in right vs left Brain, but it’s not based on behavior or personality traits.
There are some brain functions that are organized by left and right brain predominance.
For example, we know that contracting a muscle on the left side uses mostly the right motor cortex. We know that perceiving touch on the right side is mostly perceived by the left sensory cortex. We also know that when strokes hit these parts of the brain, we can have a paresis or loss of sensation on the opposite side of the body.
What might be less known outside of a neurology office is that language and speech is a very left brain dominant function, while visuospatial awareness and attention is a very right brain biased function.
This was also born out of studies on stroke patients who develop bizarre presentations. Where specific strokes in the left brain can leave some patients with severe speech and language deficits, while some right sided strokes can leave a patient ignoring the whole left side of their body!
The stories on these cases documented in “Phantoms in the Brain” by Ramachandran are really incredible.
As always, #neurology and #neuroscience are endlessly fascinating!
https://chiropractickeystone.com/wp-content/uploads/2021/03/Meniere’s-DIsease.png6301120Dr. Jonathan Chunghttp://chiropractorwellington.com/wp-content/uploads/2019/02/neuroplasticity-web.jpgDr. Jonathan Chung2021-03-27 13:33:212021-03-27 13:33:21Left Brain Vs. Right Brain: Myths and Facts
Most everyone knows about or has heard of the placebo effect; the seemingly magical ability for our bodies to feel better or overcome illness from a belief in a treatment that has no effect.
It’s one of the things in medicine that we are always wary of, especially when selecting treatments associated with alternative medicine. After all, no one wants to waste time, energy, or money on something that isn’t supposed to work. It feels like you’re getting scammed, even if the end result is positive.
However, there is a lesser known effect that I believe is more harmful phenomenon that isn’t being discussed enough. It’s more pervasive in the entirety of healthcare, and it’s societal ramifications can have massive implications on outcomes related to your own health.
We’re talking about the Nocebo Effect
Nocebo, No Bueno
Where positive beliefs about a treatment lead to positive health outcomes in placebo, nocebos occur when negative beliefs about a treatment or condition lead to negative health outcomes.
We don’t really think about nocebos because in the context of healthcare, we are not really encountering clinicians or practitioners who are intentionally trying to to make us feel worse. It’s just a poor business model.
Nocebos affect us in much more subtle ways. They happen when patients have false or exaggerated beliefs about a treatment, condition, or situation, and these beliefs can often come from well-intentioned providers or social media influencers.
Here are some of the examples of known nocebic responses in society:
People who think they are sensitive to MSG and feel sick after eating Chinese food with suspected MSG, but feel perfectly fine eating MSG-rich snack foods. David Chang tackles this in his series Ugly Delicious on Netflix. You can watch the clip here (Warning: uses the F-word a few times). I’m not saying that people can’t be sensitive to MSG (probably really uncommon), but if you are sensitive to MSG in Chinese food, but not Doritos, then you’re not sensitive to MSG, you’re likely expressing a nocebo.
Patients who take a placebo pill in a drug trial and hear a list of potential side effects are much more likely to experience those side effects compared to patients without hearing the side effects. [Source]
In 1998, a teacher in a Tennessee school reported a “gas-like” smell inside of a school. The school was evacuated, and the ensuing panic from a suspected gas-leak led to over 100 students/staff going to the emergency room with 38 of them being hospitalized over-night. It turns out that it was a false-alarm and no leaks or chemicals were detected so the illness was attributed to a mass psychogenic illness. [Source]
But remember this because it’s super important:
People experiencing nocebos are NOT faking their illness. Their symptoms and experiences are very real, but the cause of their pain or illness is not what they think it is.
Our minds exert extraordinary influence on our bodies, but our minds are easily fooled for the better with a placebo, or for the worse with a nocebo.
Are Doctors Creating Nocebos?
One example we see often in chiropractic are beliefs about X-ray or MRI findings. Many patients after getting X-rays and MRI show signs of disc degeneration or disc herniation. Disc herniations in particular are known to cause radiating arm and leg pain, especially in the acute phase of injury.
Doctors frequently talk about disc herniations and tell people that they can’t play sports anymore or lift heavy things because they have disc herniations.
But the evidence is overwhelming in showing disc herniations don’t necessarily cause chronic back pain. In fact, most disc herniations are completely asymptomatic!
By the time we are 50, we will all have disc degeneration, and most of us will have bulging discs and we will walk, run, and exercise fine without any pain!
A large study using MRI on patients without pain showed that common MRI findings associated with pain are present in PAIN-FREE people as we age.
But if we have taken the patient with a disc herniation and convinced them that their back is weak from herniation and to avoid exercise, we are predisposing this patient to nocebo to one of the best things for the chronic back pain patient….EXERCISE.
As clinicians and healthcare providers, we have to be extremely judicious with our words when interacting with patients. We are responsible for knowing when something has life altering consequences and making the appropriate recommendation for care. On the flip side, we have to be informed and know when a diagnosis is probably self-limiting and allow the patient to feel empowered that they’re going to get better; with or without our help.
Combating Nocebos
None of us are immune to the effects placebo or nocebo because of the powerful influence that beliefs have on human physiology. Our brains love to create patterns out of noise in order to make sense of the world, and the easiest way to make sense of the world is when our perception matches our beliefs.
It is important that we have strategies that reduce the impact of nocebo because nocebos can decrease your ability to recover from chronic pain and illness.
I’ve seen so many patients come into the office that have become so scared of normal human behavior that they may as well wrap themselves in bubble wrap.
This isn’t a way for a human being to live.
So how do we counter the effects of nocebo? Here are some major factors I’ve seen in practice:
Never Make Your Diagnosis Your Identity: You would never willingly allow someone to steal your credit card and social security card, but you should be even more protective about what you allow to identify as yourself. When people make their diagnosis their identity, they become resigned to accept all of the possible negative consequences of their diagnosis as an inevitable part of their life.
Embrace the Idea That Your Body Is Resilient: One of the first things we teach patients in our office is that their body is capable of healing itself. Having a belief system that your body is capable of facing challenge and enduring allows people to have a condition or illness and not allow the condition to hold them back.
Don’t Trust Health Providers That Scare You Into Treatment: It’s one of my biggest pet peeves in the world when I hear other providers using a patient’s condition to scare and coerce people into procedures. I having patients coming in each week that have doctors telling them that a small herniation is a risk for paralysis if they get into another accident and that the only solution is surgery. I’ve also had patients whose chiropractor told them that they had the worst spine they’ve ever seen because they had some signs of age related disc degeneration on their X-ray. This. Is. MADNESS
As healthcare providers, we have to ensure that our words don’t compromise the ability for a patient to get better. When we use fear and scare tactics to coerce people into taking treatment plans, we not only abusing patient trust for financial gain, you are also compromising the outcomes of patients who simply want to get better.
We have to do better and help all of our patients combat this insidious plague on our patients by empowering people to have faith and confidence in their ability to heal.
https://chiropractickeystone.com/wp-content/uploads/2020/02/ADC7E8B9-BC20-4730-99A5-6B6C0DB570B7.png21602160Dr. Jonathan Chunghttp://chiropractorwellington.com/wp-content/uploads/2019/02/neuroplasticity-web.jpgDr. Jonathan Chung2020-02-04 17:58:362020-02-04 18:07:41The Nocebo Effect: When Our Words and Beliefs Make Us Sick
2016 continues to be a troublesome year for football as science reveals more information about the effects of repetitive head contact on the brain. It’s pretty well established that concussions can create lasting changes in the structure of the brain, in recent years scientists have sought to study if contact sports can change the brain even without concussion.
Two studies presented this year sought to answer that question, and it looks like football without concussions can still affect a young and developing brain. Here are some links to studies below:
Both of these studies had a similar design, but they were performed on different age groups. One was performed on players between the ages of 8-13, the other was performed on high school players. Players were given special helmets to quantify how much head impact they were receiving in practices and in games. The players were also scanned with a special form of MRI called diffusion tensor imaging (DTI) before the season and after the season to see if there were any changes in the structure of the brain after the season.
About DTI
DTI helps to measure structural damage to the brain by helping doctors look at a part of a neuron called an axon. Axons are like power lines of a nerve cell. Whenever a neuron fires, it transmits an electrical signal down these wires so that it can pass the message along to the next neuron in the chain. DTI measures the continuous movement of water through these “wires”.
The resulting image is actually something quite beautiful and remarkable to see. Almost like something you can hang in an art exhibition as you can see below:
DTI Image of the axons in the brain. Image Credit: Google Creative Commons
One of the things that has been well established is that concussions can damage a lot of the axons in the brain through a process called axonal shearing. It’s basically like a hurricane coming in and knocking down your town’s power lines.
Image credit to Artery Studios via Pineterest Arterystudios.com
When these axons get damaged, that beautiful DTI image that you saw before hand will start to show some gaps like you see below:
Back to Football and Young Brains
So we know that concussions definitely cause axonal injury, but what about all those hits to the head that happen without a concussion? Could they also damage these axons?
According to these 2 recent studies, a year of youth or high school football can make observable changes in the structure of the brain.
The studies also showed that the players who had impacts that were more frequent or more forceful correlated with greater signs of damage.
In high school athletes, the researchers also measured functional changes in the brain and showed that players with greater or more frequent impact showed decreased delta wave activity which is a characteristic sign of brain injury.
So far, not so good.
Imaging Is Not A Death Sentence
So before we draw any conclusions, let’s talk about 2 things.
1st these were small studies looking at 1 year of football. Bigger studies and longer studies are needed to make stronger conclusions
2nd I’ve frequently talked about how you are not your imaging findings. You can look at that article here:
While we know that these DTI findings are related to concussion and head impact diagnosis, we have no idea if this means anything for the health and quality of life of the patient in the future.
Findings on DTI are NOT predictive of how impaired a patient is, nor does it predict if a patient will have future brain damage or post concussion syndrome. In fact, findings on DTI don’t predict all that much at this point in time.
Obviously we prefer that brains don’t suffer any damage at all, but we do know this:
Most people who suffer head impact and concussions will go on to live normal healthy lives.
Now it’s up to science to figure out how much can someone’s brain take, and how do we take care of these people who are at risk for future brain disease.
https://chiropractickeystone.com/wp-content/uploads/2016/12/young-brain-and-football.png315560Dr. Jonathan Chunghttp://chiropractorwellington.com/wp-content/uploads/2019/02/neuroplasticity-web.jpgDr. Jonathan Chung2016-12-13 04:40:032022-09-21 13:04:26One Season of Football and the Developing Brain